
Is your child a mouth breather?
Does your child snore, sleep with his/her mouth open, drool on the pillow and faces frequent or intermittent nasal obstruction? Or maybe he/she faces a combination of all these things?
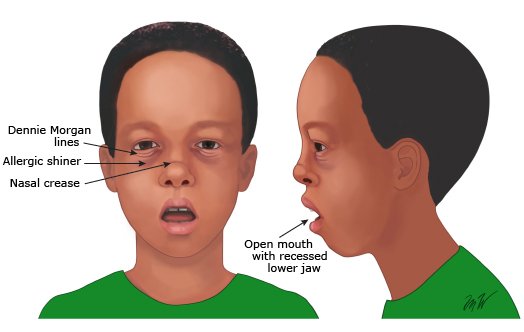
The mouth-breathing (MB) syndrome occurs when nasal breathing is substituted by a breathing pattern in which the nose is supplemented by oral respiration. (Opens mouth to take in air)

What are the causes?
It may be related to genetic factors, incorrect oral habits or nasal obstruction of variable severity and duration.
All immunologically healthy children have adenoids from birth, which reach peak growth between 4 and 5 years of age and then undergo a process of atrophy, (they disappear) which is complete at around 10 years of age. In some cases, the adenoids may increase in size to the extent that they partially or totally abstract nasal respiration. Similarly, the tonsils may increase in size to the point at which they invade the nasopharynx or extend downwards into the region of the hypopharynx.
Reducible hypertrophy (over growth) of the adenoids (HA) and/or tonsils causes obstructive forms of mouth-breathing, otitis media (inflammation of the middle ear), sinusitis and nasopharyngitis.
This is considered the primary cause of sleep-related respiratory disorders (Sleep Apnea) and compromises children’s physical and cognitive development. Children who are chronic mouth breathers may develop speech disorders, facial deformities and abnormal body posture and inadequate positioning of the teeth.
Can allergies or Bad air cause Mouth breathing?
Among the different forms of rhinitis, (inflammation of the nasal membrane) allergic rhinitis (AR) has been identified as one of the most important causes of chronic mouth breathing in growing children and does not only affect normal development of the facial skeleton but also significantly interferes with overall health, asthma control and quality of life. Ensuring that the child develops less allergies can reduce the chances of mouth breathing.

Skeletal Changes
Mouth breathing can cause underdevelopment of the jaw in children.
The temporomandibular joint may get adversely affected along with palatal stenosis in children with nasal obstruction thereby leading to airway stenosis (abnormal narrowing of a passage). The mandible gets rotated downward and backward giving the face a long narrow face (Adenoid faces).
Dental Changes
The upper anterior teeth show a tendency for labial (flaring out) inclination. This may be caused by an imbalance in the internal and external muscle force due to the lips opening. (Image-A)
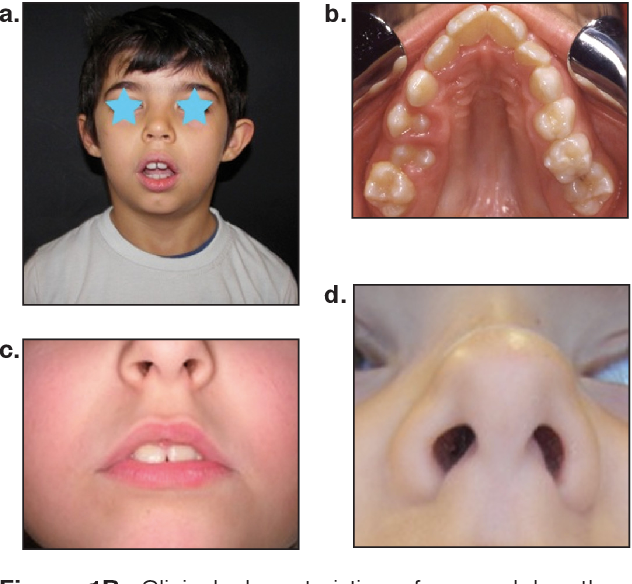
Mouth breathers usually have a narrow high arched palate (Image -B) which in turn reduces the space in the nasal cavity (Image-D) and thus less air gets circulated for breathing.
This is referred to Sleep Apnea or Obstructive Sleep Apnea where in the individual gets less oxygen while sleeping. They also face issues while playing sports or even running as less air is available to them for breathing.
Can this be corrected? When should I visit the dentist?
This can most definitely get corrected. Once a parent or a care giver sees the mentioned signs, it’s best to visit a dentist and get a detailed consultation regarding the same.
By correcting poor breathing patterns, children’s facial development can be improved to a large extent.
Surgical intervention to remove the cause, and early orthodontic treatment for malocclusion can provide children and adolescents with a higher quality of life. Timely attention to mouth breathing caused by adenoid hypertrophy and other causes can promote the physical and mental health of children.
